The Renin-Angiotensin-Aldosterone System: Pathway and Steps
Use this memory trick to remember the renin-angiotensin-aldosterone system (RAAS) and the effects it has on the body. Step-by-step guide of the RAAS pathway using flow charts, diagrams, practical applications, and tricks to remember all the components.
Disclaimer: This lecture is protected by copyright and intended for educational use only, not medical advice.
No part of this lecture or its images may be reproduced or altered in any form, etc. without written permission from Simplico.
You may share the URL to this lecture with others, provided it remains unaltered and is not used in any misleading, harmful, defamatory context, etc.
Become a Member!
Join now to access our online members-only page featuring a growing library of study guides, notes, and cheat sheets!
Get instant access to ALL our study guides, notes, and cheat sheets!
Example Case
A male patient presents with right upper quadrant abdominal pain for the past 2 days. Right upper quadrant ultrasound reveals acute cholecystitis. He is not scheduled to go to the OR until later, and you notice that he is becoming more hypotensive. In addition to expediting his surgery, he is also receiving IV antibiotics and fluids.
You perform a chart review and notice he takes lisinopril, losartan, and spironolactone. He informs you that he took all of his medications earlier that morning. You are trying to recall the pharmacodynamics of each medication and how they will impact his body’s physiological response to improve his blood pressure.
Renin-Angiotensin-Aldosterone System
You have a hypotensive patient.
What physiological responses occur in the patient to improve their hypotension?
There are several neurotransmitters and hormones released to improve perfusion to organs:
Norepinephrine
Epinephrine
Vasopressin (antidiuretic hormone)
Aldosterone
Angiotensin II
The above neurotransmitters and hormones function to improve blood pressure and perfusion through various mechanisms of:
Vasoconstriction
Increased cardiac output and/or
Sodium and water reabsorption from the kidneys
Norepinephrine and epinephrine release is influenced mainly by the sympathetic nervous system.
Whereas angiotensin II, aldosterone, and vasopressin release is influenced mainly by the renin-angiotensin-aldosterone system (RAAS).
The focus of today’s lecture will be on the RAAS and its downstream effects.
As with most of our lectures, there is a memory trick to help you remember the RAAS, its components, and what they do.
It is also recommended to view the blood pressure regulation for hypotension lecture, as it ties together the synergistic effects that the sympathetic nervous system and RAAS have to improve blood pressure and perfusion.
There will be future pharmacology lectures on ACE inhibitors, ARBs, and aldosterone antagonists.
Since the pharmacodynamics of these medications involve inhibition of various components of the RAAS, this lecture will serve as a strong foundation to easily summarize the RAAS.
RAAS Activation
The main purpose of the RAAS is to control blood pressure by regulating systemic vascular resistance, intravascular volume, and electrolytes.
Activation of the RAAS ultimately increases blood pressure through vasoconstriction as well as fluid and sodium reabsorption from the kidneys.
There are 3 main mechanisms in which the RAAS can be activated:
Sympathetic nervous system stimulation
Carotid baroreceptor detection of decreased intravascular pressure
Renal detection of decreased renal perfusion or hyponatremia
First, the function of the sympathetic nervous system is to produce a fight or flight response that increases blood pressure and organ perfusion, among other effects.
The RAAS is activated when the sympathetic nervous system stimulates beta adrenergic receptors on the juxtaglomerular cells in the kidneys to release renin, the first step in the RAAS.
Second, when carotid baroreceptors detect decreased intravascular pressure, the sympathetic nervous system is activated. This will in turn activate the RAAS as described above.
Third, the kidneys can activate the RAAS in the presence of decreased renal perfusion, decreased glomerular filtration rate (GFR), or decreased intravascular sodium chloride levels.
A decrease in any of the above will stimulate the proximal tubule of the nephron to reabsorb sodium back into the vasculature in order to help improve blood pressure, perfusion, and/or fluid and electrolyte imbalances.
An increase in proximal tubule sodium reabsorption leads to decreased sodium and chloride levels within the renal tubular system distally.
The macula densa cells in the distal tubule sense the decreased sodium and chloride levels and will activate the RAAS as a result.
3 Main Mechanisms for Activating the RAAS
Sympathetic Nervous System (SNS) - The SNS acts on beta-1 receptors in the kidney to release renin, the first step in the RAAS.
Carotid Baroreceptors - Carotid baroreceptors detect decreased intravascular pressure which will activate the SNS and RAAS.
Kidneys - Kidneys detect decreased renal perfusion or low sodium chloride levels and will activate the RAAS.
Below are illustrations depicting the 3 mechanisms for activating the RAAS described above.
The first step in the RAAS is renin release from the juxtaglomerular cells of the kidneys.
This will be discussed in more detail below, however, you will see the following illustrations show this first step.
Sympathetic Nervous System (SNS) - The SNS increases levels of norepinephrine (NE) and epinephrine (EPI) that bind to beta-1 receptors on the kidneys.
Increased sympathetic activity will cause postsynaptic sympathetic neurons to release norepinephrine, and the adrenal medullae to release epinephrine and norepinephrine into the blood stream.
Juxtaglomerular cells in the kidney express these beta-1 receptors, and they release renin as a result of catecholamines binding to it.
Norepinephrine (NE) released by postsynaptic sympathetic neurons, and epinephrine (EPI) and norepinephrine released by the adrenal medulla from sympathetic activity bind to beta-1 adrenergic receptors on the juxtaglomerular (JG) cells. This causes renin release.
Carotid Baroreceptors - Carotid baroreceptors activate the SNS in the presence of decreased intravascular pressure. The SNS causes the JG cells to release renin as described in the first illustration above.
Kidneys - The kidneys detect when there is decreased renal perfusion or decreased intravascular sodium chloride levels.
This will increase sodium and chloride reabsorption from the proximal tubule back into the vasculature.
As a result, there is decreased sodium and chloride levels in the distal renal tubule.
Macula densa cells (yellow circles) in the distal tubule sense the decreased renal tubular sodium and chloride levels, and will stimulate JG cells to release renin; the first step in the RAAS.
From RAAS Activation to Angiotensin II
Now that we know how the RAAS is activated, let’s discuss the next steps that occur.
Angiotensin II is the main player in the RAAS that facilitates all the downstream physiological effects to increase blood pressure and improve fluid or electrolyte imbalances.
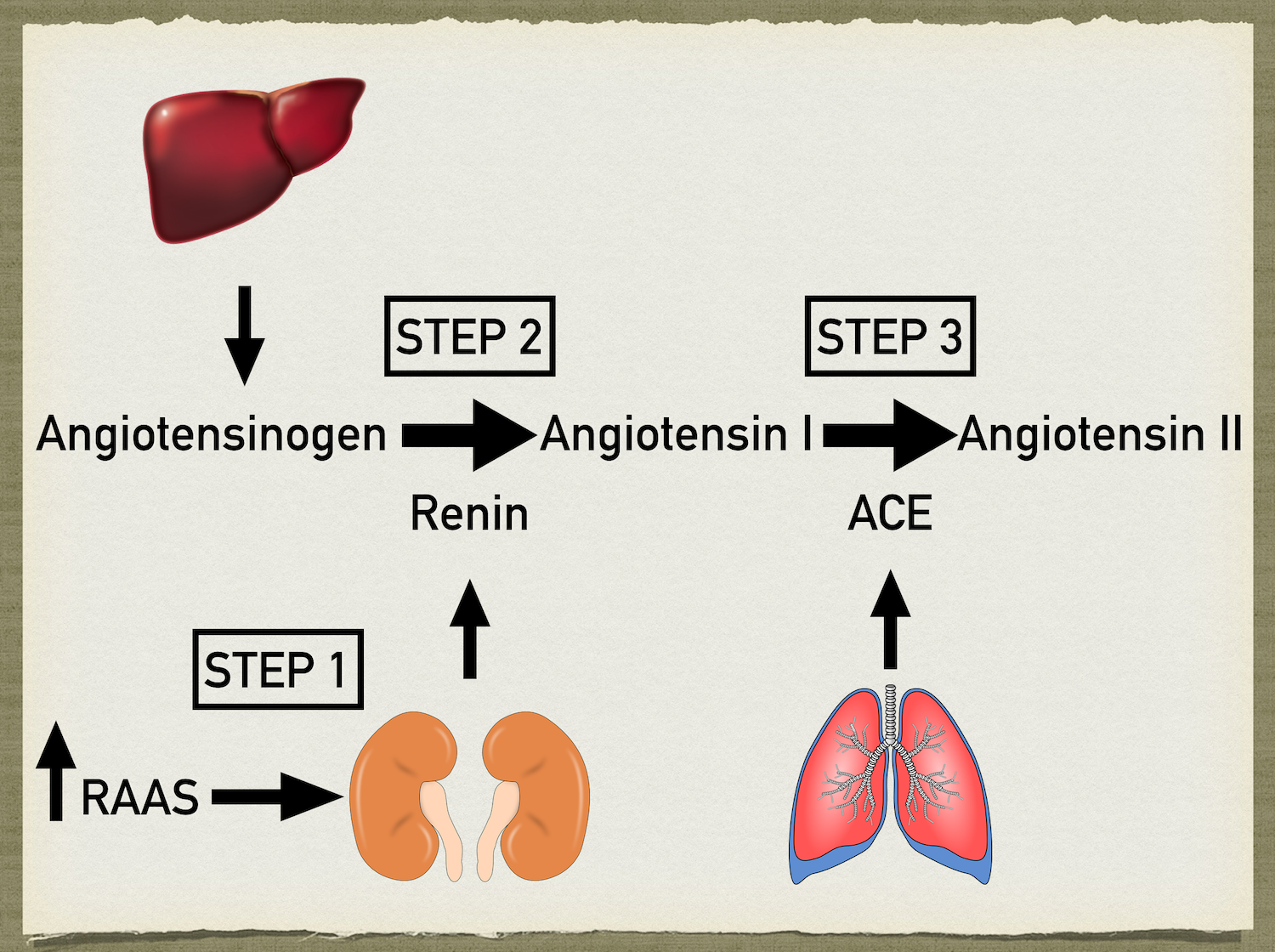
There are 3 main steps that occur to produce angiotensin II: renin release, conversion of angiotensinogen to angiotensin I using renin, and conversion of angiotensin I to angiotensin II using angiotensin converting enzyme (ACE).
Step 1: Renin Release
The first step that occurs once the RAAS is activated by one of the mechanisms above (sympathetic activation, carotid baroreceptors, or renal induced activation) is renin release from the juxtaglomerular (JG) cells of the kidneys.
The JG cells express beta-1 adrenergic receptors and are therefore directly activated by the sympathetic nervous system to release renin.
The JG cells are also stimulated to release renin when the macula densa cells of the distal tubule detect decreased renal tubular sodium and chloride levels.
Step 1: Activation of the RAAS causes renin release from the JG cells of the kidneys.
Step 2: Angiotensinogen into Angiotensin I
Angiotensinogen is a globular protein produced and released by the liver. Renin is an enzyme that functions to cleave angiotensinogen to form angiotensin I.
Step 2: Renin cleaves angiotensinogen (released by the liver) to form angiotensin I.
Step 3: Angiotensin I into Angiotensin II
As mentioned above it is angiotensin II, not angiotensin I, that is the active component of the RAAS for facilitating blood pressure regulation.
Therefore, angiotensin I needs to be converted into angiotensin II, and this is accomplished by an enzyme fittingly named angiotensin converting enzyme (ACE).
This enzyme is mainly found within the lungs.
We now have angiotensin II which has multiple downstream effects to improve blood pressure, fluid imbalance, and electrolyte imbalance discussed below.
Step 3: Angiotensin I is converted to angiotensin II by angiotensin converting enzyme (ACE) mainly found within the lungs.
Tricks to Remember the RAAS Components
The components discussed in the RAAS have included renin, angiotensinogen, angiotensin I, angiotensin II, and ACE.
To summarize, RAAS activation leads to renin release from the kidneys. Renin cleaves angiotensinogen, which is released by the liver, to form angiotensin I. Finally, angiotensin I is converted into angiotensin II by ACE which is found mainly within the lungs.
It can be challenging to remember all the different components, where each component is produced, and the function of each component.
Here are some memory tricks to help!
Where each component is produced:
RENin = RENal (Renin is released by the kidneys)
AngiotensinoGIN = GIN/alcohol = Liver (Angiotensinogen is released by the liver)
ACE= AIR = Lungs (ACE is found within the lungs)
Enzyme function:
Renin = cuts off the end of the word angiotensinOGEN to form angiotensin (Renin cleaves angiotensinogen to form angiotensin I)
Angiotensin CONVERTING enzyme = CONVERTS angiotensin I into angiotensin II
Effects of Angiotensin II
Angiotensin II has multiple downstream effects to regulate and increase blood pressure.
1. Angiotensin II is a potent vasoconstrictor. It acts to increase systemic vascular resistance by constricting blood vessels which in turn increases pressure.
2. Angiotensin II causes vasopressin/antidiuretic hormone (ADH) release from the posterior pituitary gland. The 2 primary actions of vasopressin is peripheral vasoconstriction and water reabsorption from the kidneys. Both of these effects will lead to increased blood pressure. These 2 actions can be easily remembered by the interchangeable hormone name. Vasopressin = vasoconstriction. Antidiuretic hormone = antidiuretic.
3. In addition to the release of vasopressin from the posterior pituitary gland, angiotensin II also causes aldosterone release from the adrenal cortex. Aldosterone acts on the distal renal tubule to reabsorb water and sodium, thereby increasing blood volume and blood pressure.
4. In addition to ADH and aldosterone induced fluid and sodium reabsorption from the kidney, angiotensin II also directly acts on the kidney to reabsorb sodium by stimulating the Na+/H+ channels in the proximal tubule. It also constricts efferent arterioles in the kidney to maintain adequate GFR. This will lead to decreased plasma fluid downstream of the efferent arterioles thus further augmenting sodium and fluid reabsorption from the renal tubules.
5. Angiotensin II acts to increase sympathetic surge. It acts centrally to increase sympathetic outflow, and also acts peripherally on sympathetic ganglia and the adrenal medulla to facilitate sympathetic response.
Angiotensin II Effects
Vasoconstriction
Vasopressin/Antidiuretic Hormone (ADH) Release
Directly acts on kidneys to reabsorb sodium and fluid, efferent arteriole constriction
Aldosterone Release
Increase Sympathetic Outflow
Angiotensin II effects include (1) direct vasoconstriction, (2) antidiuretic hormone (ADH)/vasopressin release leading to vasoconstriction and renal tubule water reabsorption, (3) direct stimulation of kidneys to reabsorb sodium and constrict efferent arterioles, (4) aldosterone release leading to sodium and water reabsorption, and (5) increased sympathetic outflow.
***Tubule and efferent arteriole illustrations above are simplified for purposes of focusing on angiotensin II effects. It does not accurately depict what part of the tubule each component targets. For example, aldosterone acts on the distal tubule, ADH on the collecting ducts, and angiotensin II on the proximal tubule.
Everything you need to know about the nephron can be learned in 5 easy steps.
Practical Application
As described above, there are multiple steps in the RAAS.
This creates several targets for medications.
You can appreciate how medications such as ACE inhibitors, angiotensin II receptor blockers (ARBs), and aldosterone antagonists can be useful in treating hypertension, CHF, or renal complications from diabetes.
For more information about the mechanism of action, indications, side effects, and contraindications of ACE inhibitors, check out the ACE Inhibitor lecture!
Summary
Hopefully that helped clarify or refresh your memory of the RAAS.
The RAAS is activated via sympathetic activity, carotid baroreceptor detection of decreased intravascular pressure, and renal detection of decreased perfusion or hyponatremia.
Below is a summary slide of the 3 steps of the RAAS: Renin release, angiotensinogen conversion to angiotensin I, and angiotensin I conversion to angiotensin II.
The angiotensin II downstream effects to increase blood pressure and blood volume include vasoconstriction, aldosterone release, vasopressin release, renal tubular sodium and water reabsorption, and sympathetic surge augmentation.